
Blue Lights for a Blue Man
“A 24 year old Man was brought into ED by ambulance after being found unresponsive at home by his Girlfriend.
He had been out with mates the night before and returned in the early morning intoxicated with alcohol and cocaine.
He appeared ‘slate blue’ in colour with RR 40, sats 85% 15L NRBM, HR 110, BP 150/90, GCS 8, T 37.1, BSL 18.”
VBG
pH 7.07
pCO2 58
pO2 20
HCO3 16
BE -12.4
K+ 6.3
Chloride 114
Glucose 19
Lac >20
OxyHb 12.0%
Deoxyc Hb 0.0%
CarboxyHb 4.2%
MetHb 63.9%
“He was diagnosed with methaemaglobinaemia secondary to likely benzocaine ingestion (used as a cutting agent in cocaine). He was treated with methylene blue and intubated for low GCS, then transferred to ICU where he was extubated successfully the next day.”
Key Learning Points
Technical:
- Diagnosis
Methaemoglobinaemia occurs when ferrous ions (Fe2+) of haem are oxidized to the ferrous state (Fe3+) and then cannot bind to O2
People may present with knowledge of a congenital methaemaglobinaemia but most acute cases are caused by ingestion of a toxin:
- aniline dyes
- benzene derivatives
- chloroquine
- dapsone
- prilocaine
- metoclopramide
- nitrites (nitroglycerin, NO, sodium nitroprusside, sodium nitrate)
- sulphonamides
Suspect if patient presents with suspicion of toxic ingestion plus altered mental status, blue/grey cyanotic skin, poor O2 sats unresponsive to O2 administration (classically 85%) and brown/’chocolate’ coloured blood
- Treatment
Treat with usual supportive treatment/ resuscitation and follow usual ACLS protocol
Give methylene blue 1-2mg/kg IV stat – this can now be found in the resus drug cupboard
It comes in 50mg/5ml ampoules and should be given neat at 0.1-0.2ml/kg and then repeated once at 30-60mins if MetHb levels are not falling
Call poisons for advice early on 13 11 26
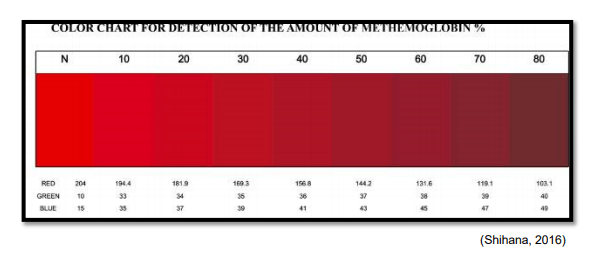
Remember when MetHb concentrations are ‘massive’ you may get an ‘error’ reading on your VBG result. In this case, use the colour chart for the estimation of the MetHb concentration in blood
Non-Technical
- Utilise available resources
Protocols for the administration of IV drugs can be found on the L drive: Emergency -> Public -> Clinical Policies and Procedures -> Pharmacology -> Emergency and Intensive Care drug Protocols
Call poisons early on 13 11 26
- Communication
Telephone calls to poisons or other specialists: Make sure you know what you are asking for. Is it for hands-on assistance? Or for specific management advice. The team leader should brief you prior to making the call but if you are ensure, feel empowered to ask.
Regular summaries enable the team as a whole to take stock of the current situation and allows the team leader to share his/her clinical reasoning and priorities with the team. It also allows for questions or concerns to be raised by team members.
Ensure all key information is fed back to the team leader and all key decisions are communicated via the team leader. This is especially important when there is more than one senior clinician in the team who may be making decisions. Remember the team leader is the only team member with complete cognitive oversight of the situation.



Leave a comment