Communication skills in high acuity situations: Team, Patient, Consultation
The bat phone rings at 10 o’clock on a chilly Tuesday morning in your ED. You huddle for warmth around the radio with your resuscitation team…
The paramedics are bringing a 58 year old lady with an episode of syncope this morning and increasing shortness of breath over 2 days. She has a background of metastatic lung cancer.
Vital signs: RR 28, Sats 97% r/a, HR 112, BP 88/56, T 36.7, GCS 15.
The patient arrives and is alert, ‘chipper’ and able to give a comprehensive history. You request an ECG, VBG and CXR and perform a bedside echo, which demonstrates a large pericardial effusion with signs of cardiac tamponade.
You smoothly coordinate your team to stabilise the patient, ascertain her treatment goals and request specialist interventional cardiology consultation with the end goal of transferring her to the interventional suite for pericardial drainage.
She recovers well and is discharged home a few days later to meet her new Granddaughter born the following week.
We discussed the following learning points in debrief:
Optimise your team’s performance through effective use of the pre-arrival time
Brief your team as a whole involving medical and nursing team together
Use a structured communication tool for preparing your team for a resuscitation for example the “Team Briefing Model”, see link below
Consider asking all team members to verbalise their roles and priorities to one another prior to the patients’ arrival
Use the opportunity to reinforce mutual respect amongst team members to encourage speaking up and making suggestions
Even though it’s a resuscitation, allow the patient opportunity to set their own agenda
It is natural to want to use closed questions in a high acuity situation to establish facts, highlight red flags and rapidly rule in and out potential differentials. Evidence shows that open questions gather more information, more quickly than closed questions. And you will very quickly establish your patient’s main concerns, ideas and expectations
When consulting specialists over the phone use a structured approach, be polite and collaberative and most of all, be honest!
Use a telephone consult structuring tool such as CONSULT or 5 Cs (see below)
At night, allow at least a minute for the phone call recipient to wake up. Fill this time by politely introducing yourself (name, role, level of experience, location), checking who you are speaking to and giving details of the patient you are calling to discuss
Quickly move on to the key question, which should be specific, focused and brief. Examples: “I need you to come in urgently to assist with xyz”; “I need your advice on whether to intubate the patient with hypercapnic respiratory failure and advanced, end stage COPD”; “I need you to come in to drain a pericardial effusion causing cardiac tamponade”
Don’t panic if you can’t answer some of the more technical questions the specialist may ask. Be honest, don’t lie. Re-iterate your level of experience and your primary question
Today in JMO teaching we talked about the management of acute heart failure in the ED, specifically the management of acute pulmonary oedema or “SCAPE” (Sympathetic Crashing Acute Pulmonary Edema).
I have attached the clinical vignette, tutorial notes and some interesting references for further reading.
FIBs, medical error, resuscitation directives and ‘where the *@#! is the intralipid’?!
It is an eerily quiet Tuesday morning in ED. You have just returned from a coffee round to hear the arrest buzzer sound from bed 18. Edna is 89 and is currently unresponsive after an inadvertent intravascular administration of ropivacaine in an effort to analgese her fractured NOF.
She is unresponsive, hypotensive and tachycardic with a broad, erratic rhythm on the monitor. She subsequently suffers a generalised seizure, following which she becomes apnoeic and arrests into pulseless VT.
You commence ALS, successfully resuscitate her with sodium bicarb and IV lipid emulsion and transfer her to ICU to await her total hip replacement.
Key Learning Points: Technical
Local Anaesthetic toxicity is real! Know weight-based maximum doses and fully consent patients/family for complications prior to undertaking any procedure.
Manifestations result from sodium channel blockade and include neurological sequelae including tinnitus, perioral numbness, confusion, drowsiness, loss of consciousness and seizures, closely followed by cardiovascular complications including hypotension, dysrhythmias and cardiac arrest.
The key investigation is the 12-lead ECG, which may show signs of Na+ channel blockade: terminal R >3mm in aVR, broad QRS >100ms in II, R/S ratio >0.7 in aVR.
Treat dysrhythmias with sodium bicarb eg 2mmol/kgl IV bolus and repeat until cardiac stability is restored.
In refractory arrest, use IV lipid emulsion 1-1.5ml/kg bolus repeat at 3-5mins x 1-2 then 0.25ml/kg/min IVI.
Lipid emulsion 20% can be found in the drug cupboard in AAA, resus and fast track. Dosing information should be attached to the bottle but if not (as in this case!) please contact poisons for advice.
Key Learning Points: Non-Technical
Role allocation can be very tricky when a critically ill patient is sprung upon us, outside of a familiar resus environment. Have a plan to manage role delineation on-the-fly. Consider pausing to allocate roles; use labels eg stickers/lanyards in acute situations even outside of resus – perhaps keep some on the resus trolleys for this reason. Allocating roles ensures team members are accountable and focused and ensures important tasks are not missed eg time-keeping, drug-drawing.
Communicate with and listen to the Team Leader. They will use key phrases to update the team in language that is universally understood. For example, ‘I think we are dealing with local anaesthetic toxicity’, ‘I want to prioritise the IV lipid emulsion’. Use closed-loop communication to inform the TL that tasks have been completed, ‘the defib pads are on, shall I proceed with rhythm check?’.
Feel empowered as a team member to speak up if you know something that you feel the rest of the team has overlooked eg the location of important medications in the department. As the TL be open to suggestions and regularly update your team and invite feedback so as to avoid lost communication of vital information.
Think about the ethics around over-riding a ‘do-not-resuscitate’ directive in the event of an unexpected, iatrogenic event. If it is clear the directive has been drawn-up with potential iatrogenic events in mind, the patient’s wishes should be respected. Consider incorporating this element into your advanced-care-planning discussions with family and relatives. When consenting for nerve blocks, always disclose risks of LA toxicity including possible cardiac arrest and where possible discuss with elderly, frail patients/families their wishes in the event of cardiac arrest as a result of a procedural complication. By planning in advance we can avoid fraught decision making in the heat of the moment. Remember, it is natural as care-givers to want to correct an inadvertent error by over-treatment. This is not a reasonable excuse for over-riding an advanced care directive. We must always be acting in the patient’s best interests.
Today Brigitte the palliative care CNC came to talk to us about palliative care services and referral processes in our area, and provide some resources to assist us with having end-of-life conversations and prescribing in palliative care.
Main learning points for me were:
We can refer to community palliative care at the time of discharge from ED by faxing a referral form, and we should be doing this if appropriate.
We do not have an out of hours on-call palliative care service currently at this hospital.
Prescribing protocols for patients requiring end-of-life medications can be found in the ‘policies and procedures’ desktop icon -> 7. Medications -> ‘Care of the imminently dying adult inpatient’. The opioid conversion chart is also found within this folder.
Starting the conversation about goals of care/ end of life wishes and needing to bail out, is better than not starting at all and will help the next person who attempts it. Don’t persevere with a conversation that is failing.
Brigitte kindly sent me some useful resources relating to today’s session. Her teaching powerpoint, some communication skills resources and community palliative care referral form can be found below.
“A 24 year old Man was brought into ED by ambulance after being found unresponsive at home by his Girlfriend.
He had been out with mates the night before and returned in the early morning intoxicated with alcohol and cocaine.
He appeared ‘slate blue’ in colour with RR 40, sats 85% 15L NRBM, HR 110, BP 150/90, GCS 8, T 37.1, BSL 18.”
VBG
pH 7.07
pCO2 58
pO2 20
HCO3 16
BE -12.4
K+ 6.3
Chloride 114
Glucose 19
Lac >20
OxyHb 12.0%
Deoxyc Hb 0.0%
CarboxyHb 4.2%
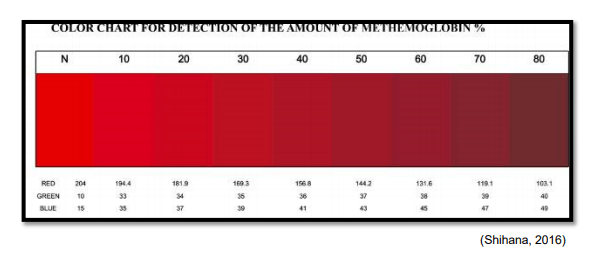
MetHb 63.9%
“He was diagnosed with methaemaglobinaemia secondary to likely benzocaine ingestion (used as a cutting agent in cocaine). He was treated with methylene blue and intubated for low GCS, then transferred to ICU where he was extubated successfully the next day.”
Key Learning Points
Technical:
Diagnosis
Methaemoglobinaemia occurs when ferrous ions (Fe2+) of haem are oxidized to the ferrous state (Fe3+) and then cannot bind to O2
People may present with knowledge of a congenital methaemaglobinaemia but most acute cases are caused by ingestion of a toxin:
aniline dyes
benzene derivatives
chloroquine
dapsone
prilocaine
metoclopramide
nitrites (nitroglycerin, NO, sodium nitroprusside, sodium nitrate)
sulphonamides
Suspect if patient presents with suspicion of toxic ingestion plus altered mental status, blue/grey cyanotic skin, poor O2 sats unresponsive to O2 administration (classically 85%) and brown/’chocolate’ coloured blood
Treatment
Treat with usual supportive treatment/ resuscitation and follow usual ACLS protocol
Give methylene blue 1-2mg/kg IV stat – this can now be found in the resus drug cupboard
It comes in 50mg/5ml ampoules and should be given neat at 0.1-0.2ml/kg and then repeated once at 30-60mins if MetHb levels are not falling
Call poisons for advice early on 13 11 26
Remember when MetHb concentrations are ‘massive’ you may get an ‘error’ reading on your VBG result. In this case, use the colour chart for the estimation of the MetHb concentration in blood
Non-Technical
Utilise available resources
Protocols for the administration of IV drugs can be found on the L drive: Emergency -> Public -> Clinical Policies and Procedures -> Pharmacology -> Emergency and Intensive Care drug Protocols
Call poisons early on 13 11 26
Communication
Telephone calls to poisons or other specialists: Make sure you know what you are asking for. Is it for hands-on assistance? Or for specific management advice. The team leader should brief you prior to making the call but if you are ensure, feel empowered to ask.
Regular summaries enable the team as a whole to take stock of the current situation and allows the team leader to share his/her clinical reasoning and priorities with the team. It also allows for questions or concerns to be raised by team members.
Ensure all key information is fed back to the team leader and all key decisions are communicated via the team leader. This is especially important when there is more than one senior clinician in the team who may be making decisions. Remember the team leader is the only team member with complete cognitive oversight of the situation.